






Guests
- Uché Blackstockemergency medicine physician, Yahoo News medical contributor, and CEO and founder of Advancing Health Equity, a company working with healthcare organizations to fight racism and bias in services.
- Sheri Finkauthor, New York Times correspondent and executive producer of the Netflix docuseries Pandemic: How to Prevent an Outbreak.
The coronavirus continues to hit communities of color the hardest, with federal data showing African American and Latinx people are nearly three times more likely to be infected and twice as likely to die from the virus compared to their white neighbors. There were “pretty significant racial health disparities” even before COVID-19 ravaged the country, says Dr. Uché Blackstock, emergency medicine physician in New York and founder and CEO of Advancing Health Equity, a company working to fight racism and bias in health services. “What we saw in the pandemic these first few months is these really significant racial health inequities being exposed and even amplified.” We also continue to speak with award-winning New York Times correspondent Dr. Sheri Fink.
Related Story
Transcript
AMY GOODMAN: This is Democracy Now! The Quarantine Report. I’m Amy Goodman, with Juan González. We’re looking at the coronavirus pandemic and disparities in treatment and in deaths. Newly released federal data shows African American and Latinx people are nearly three times more likely to be infected and twice as likely to die from the virus compared to their white neighbors. The New York Times reported these figures after suing the Centers for Disease Control and Prevention for the federal data. In April, New York City Mayor Bill de Blasio acknowledged the racial disparities in the city’s coronavirus death rates.
MAYOR BILL DE BLASIO: So, now I have information that points out that there are clear inequalities, clear disparities in how this disease is affecting the people of our city. … The deaths because of COVID-19 in the city, first and foremost, have affected the Hispanic community, with 34% of the deaths. That community is about 29% of all New Yorkers in terms of population, but 34% of the deaths. And again, this is preliminary information that we’ll keep adding to. It’s hard to talk about this stuff like statistics. This means human beings. This means families. But we have to look in the face these disparities that we’re learning about. So, the Hispanic community, 34%. The Black community, 28% of the deaths compared to about 22% of the overall population. … The disparities that have plagued this city, this nation, that are all about fundamental inequality, are once again causing such pain and causing people, innocent people, to lose their lives. It’s just abundantly clear. It’s sick. It’s troubling. It’s wrong.
AMY GOODMAN: So, that’s Mayor de Blasio speaking recently.
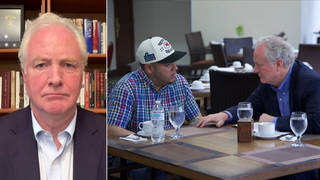
Still with us in Houston is Dr. Sheri Fink, New York Times Pulitzer Prize-winning journalist, who recently co-wrote a piece headlined “Why Surviving the Virus Might Come Down to Which Hospital Admits You.”
We are also joined by Dr. Uché Blackstock, emergency medicine physician, and CEO and founder of Advancing Health Equity, a company that works with healthcare organizations to fight racism and bias in services.
Dr. Blackstock, thanks so much for joining us, as well. If you can talk about the disparities — who lives, who dies, and who gets sick, and who doesn’t?
DR. UCHÉ BLACKSTOCK: Sure. You know, I think that before the pandemic, what people may not realize is that there were pretty significant racial health disparities in this country. I think many people had heard about the Black maternal mortality crisis, that had gotten a lot of press. But what we saw in the pandemic these first few months is these really significant racial health inequities being exposed and even amplified.
We saw that Black and Latinx and Indigenous communities were more likely to be infected because they were essentially placed at risk given the types of jobs that they had. They were more likely to be essential workers and service workers. These were public-facing jobs. They were essentially exposed. They were also more likely to use public transportation in urban areas and more likely to live in overcrowded housing. These are all risk factors for being infected with the disease. And then, to think about which communities carry the highest burden of chronic diseases, diabetes, high blood pressure, obesity and asthma are all risk factors for doing very poorly when you are infected with coronavirus. And so, those are some of the factors for why we’re seeing Black, Latinx and Indigenous communities being so disproportionately impacted by this pandemic.
JUAN GONZÁLEZ: Dr. Blackstock, I’d like to ask you specifically in terms of some of the figures I’ve seen in terms of the Latino community — for instance, here in New Jersey, 19% of the population, 30% of the COVID cases; in Utah, 14% of the population, 42% of the COVID cases. This whole issue, because the Latino community, generally speaking, is a much younger community than either the African American or the white community, so you would — the proportion that are elderly are much smaller. Is this more a function of the underlying conditions that affect the community — for instance, diabetes and other underlying conditions in the community? Or is this — what other factors do you see affecting the Latino rate?
DR. UCHÉ BLACKSTOCK: Right. And so, you know, as I mentioned, I think when we talk about who is at risk for being infected, it also depends on who is at risk for being exposed. And so, I think that those numbers that you cite point to the fact that Latino community members are more likely to be working in jobs where they’re at risk for being exposed. And, of course, this is because of practices and policies that limit certain racial groups to certain types of jobs.
And so, I think that what we’re seeing really are the outcomes of structural racism in this country. We have seen how life opportunities, including jobs opportunities, educational opportunities, have basically limited people and put people at risk to being in situations where they are more likely to be infected with coronavirus. And what I found very interesting about The New York Times piece was that we’re not just seeing it in urban areas. We’re seeing it in rural areas, right? So I would say that that speaks to the expansive reach of racism in this country.
AMY GOODMAN: You wrote a piece, Dr. Uché Blackstock, in The Washington Post headlined “Community health workers are essential in this crisis. We need more of them.” In it, you suggest community health workers are essential to addressing this issue of systemic racism. Explain.
DR. UCHÉ BLACKSTOCK: You know, I think that what we are seeing is that Black, Latinx, Indigenous communities need to be really centered in this pandemic. Right? They’re the communities being most disproportionately impacted. And I think a key part of that is messaging and outreach. And who better to do that than people who are from those communities, trusted individuals who know the nuances of what messaging entails? And so, for example, when you are contact tracing somebody and you approach that person, you have to ask them, “Which people have you been in contact with?” And for someone who may be undocumented, to be able to give out that information, you have to trust the person who’s asking you that. So I think community health workers really have a significant role to play in this pandemic, especially in relation to mitigating the impact of this virus on racialized minority communities.
JUAN GONZÁLEZ: I’d like to bring Dr. Sheri Fink back into the conversation and ask you a question about the numbers we’re seeing in terms of the deaths from coronavirus. While the number of confirmed cases is spiraling, the defenders of President Trump say, “Well, the death rate has been going down.” I mean, on a daily basis, it’s still relatively high, in the hundreds, but certainly not at the level it was earlier this year when it was in the thousands. Your sense of this shift between the confirmed cases versus deaths?
DR. SHERI FINK: Yeah. Well, that’s a positive thing, certainly. We are seeing the hospitals very overstretched here in Houston. And I asked that question about the deaths. And, of course, nobody knows for sure. But some of the factors that may be contributing to the deaths being lower, number one, the younger patient population with this — well, won’t say “wave,” it’s considered the same wave, but this surge of patients is generally younger. They have better outcomes. Number two, there are things that — you know, doctors have been sharing knowledge, science has been advancing, and so there are some treatments that seem to be effective. So, the physicians, the nurses, they feel that they’re able to care for the patients better. That may be contributing to these better outcomes.
The concern is that if the people who are younger are then going to pass the virus on to the older patient — or, the older population, then we may see some of this shift. And the other thing is that, from infection to getting sick to getting hospital sick, if you’re going to, and then to getting critically ill, there’s a lag time of weeks in between those. So even as we hopefully start to see some numbers of new infections go down or flatten, that it could be many weeks later before you know the true death toll. But the good news is, it does — there are signals it does look like it is lower at this time.
AMY GOODMAN: Sheri Fink, I wanted to go to this piece that you wrote, “Why Surviving the Virus Might Come Down to Which Hospital Admits You.” This was a piece about New York City, about public hospitals and private hospitals. The door you go through, you know, which hospital, can determine whether you live or die. Explain.
DR. SHERI FINK: So, a number of doctors got a hold of some of us reporters, and they were doctors who work in multiple campuses, different hospitals. Sometimes they rotate in the private system and in the public system. And they were concerned because they felt that there were differences. And some of them got data, raw data, mortality, so the percentage of deaths, to put it simply. And there were vast differences at one campus versus another.
And so, they felt that there were differences in care, too. Nursing ratios were much worse at some hospitals than others, and that’s very, very important. So the number of patients that a nurse has, when a nurse is the one who’s really monitoring that patient and able to see if they suddenly take a turn for the worse, which happens with this disease, those ratios were incredibly large, the number of patients per nurse as at some hospitals.
There were also modalities of treatment. So, for example, I spent a lot of time at the Brooklyn Hospital Center, this wonderful community hospital that has — in Fort Greene, New York, in Brooklyn, that has no parent company, no larger system, so they’re nimble, they’re small. But they also don’t do things that some of the bigger hospital systems do, the really sort of — ECMO, for example, this heart-lung machine, if you’re really, really, really sick. They don’t do continuous dialysis there, which is a form of dialysis that is sometimes used in critical care patients. So, it’s all to say that there are differences in the care.
And as Dr. Blackstock said, these are preexisting differences in our healthcare system, which is very unequal in New York City and likely across the country. So, because people were going to their nearest hospital, that would sort of, like, magnify or amplify it, sort of. There’s a quote in the story that this pandemic hit on top of an epidemic of these structural inequalities and racism. And so these are magnifying effects.
I will say, I want to say, an important caveat, which is that the patient populations are different that these hospitals serve. So, this is very, very important, because if you’re a hospital right near a nursing home, which some of the hospitals with the worst outcomes had, that patient population was more likely to die. They were having those underlying conditions and the higher age, that does go along with death.
So, it’s just an important signal. You know, journalism is the first draft of history. And many people who focus on health equity, like Dr. Blackstock and other researchers, are saying we have to look more into this. We have to adjust those figures. And early signs are, even when you adjust for things like age, how ill a patient is, that in fact there are important differences between hospitals that may have to do with these differences in what they can provide.
JUAN GONZÁLEZ: I’d like to ask Dr. Blackstock — we have only about a minute left, but I’m wondering your sense of this shift of the epicenter of this pandemic in the United States from the Northeast and the Midwest now to the South and the Southwest. Have you ever seen a public health crisis so politicized and so dependent on the decisions of political leaders rather than public health officials, and what the impact of that is on the Black and Brown communities?
DR. UCHÉ BLACKSTOCK: No, no. Obviously, no, I have not. And just like you, I am alarmed and appalled. You know, we’re actually in the very early stages of this pandemic, whether we believe it or not, and there are many more deaths that could actually happen. And so I think that we have an opportunity here. We have an inflection point, where we can really press on state and local officials to put interventions in place, targeted testing, contact tracing, messaging and outreach to Black and Brown communities, really to prevent further devastation to the communities that have already been so hard hit.
AMY GOODMAN: We want to thank you both for being with us. Dr. Uché Blackstock is an emergency medicine physician and CEO of Advancing Health Equity. Dr. Sheri Fink is a New York Times correspondent, Pulitzer Prize-winning journalist and writer. We’ll link to your pieces from Houston and New York City.
That does it for our show. Democracy Now! is produced with Mike Burke, Renée Feltz, Deena Guzder, Libby Rainey, Nermeen Shaikh, Carla Wills, Tami Woronoff, Charina Nadura, Sam Alcoff, Tey-Marie Astudillo, John Hamilton, Robby Karran, Hany Massoud, Adriano Contreras, María Taracena. Our general manager is Julie Crosby. Special thanks to Becca Staley, Miriam Barnard, Paul Powell, Mike DiFilippo, Miguel Nogueira, Hugh Gran, Denis Moynihan and David Prude.
Stay safe by wearing a mask. You protect yourself. You protect your family. You protect the community.
To see all the transcripts and the video and audio podcasts of Democracy Now! The Quarantine Report, go to democracynow.org. I’m Amy Goodman, with Juan González. Stay safe.



Media Options